
Breast Augmentation Education

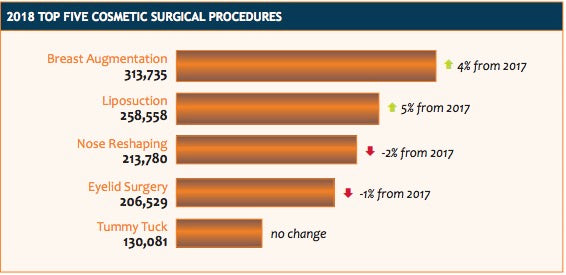
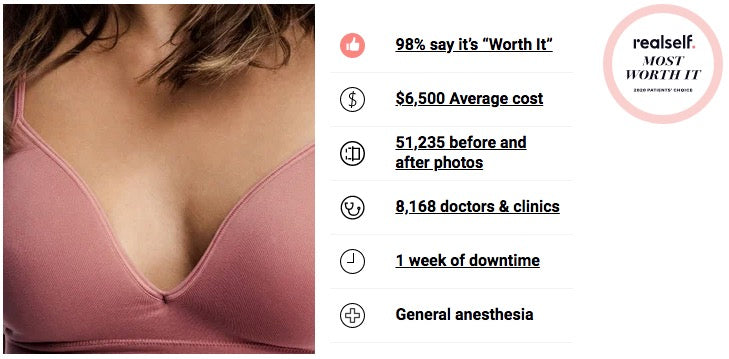
In 2018, The American Society of Plastic Surgeons reports that breast augmentation was the most popular plastic surgical procedure and has been since 2006. Satisfaction rates for breast augmentation are the highest reported in the specialty at 98%. Therefore, it comes as no surprise that the procedure with the highest satisfaction rate would also be the most popular.
Most Popular Reasons Why Women Choose Breast Augmentation
- Boost Self-Image, Self Esteem
- Disproportionately Small Breasts
- Asymmetry: Size Difference between the Breasts
- Weight Loss with Loss of Breast Size
- Pregnancy Related Changes in Breast Size and Shape
- Breast Deformities such as Tuberous Breast Shape
- Positive Impact on Sex Life
- Better Fitting Clother and More Clothing Options
- Look Younger
- Careful Consideration: The Benefits of the Procedure Outweight the Risks
Considerations when Choosing Breast Augmentation

| Implant | Size |  |
| Implant | Shape |  |
| Implant | Profiles |  |
| Implant | Pocket: Subglandular, Submuscular, Dual Plane |  |
| Incision | Breast Crease/Inframammary, Periareolar, Transaxillary, Umbilical |  |
| Implant Type | Saline |  |
| Implant Type | Silicone |  |
| Implant Type | Structured Saline |  |
Breast Implant Size
Choosing the correct breast implant size is both a scientific and aesthetic endeavor. An implant first must fit the breast dimension and then enhance volume to the desired endpoint. The most important measurement in breast implant sizing is the base width. The base width is measured from the breast attachement to the breastbone (sternum) to its lateral position near the armpit (anterior axillary line). The measurement in centimeters is the base diameter or base width.

Profile
In addition to base width, breast implants come in a variety of profiles: low, plus, moderate, high, ultra high. For a given base width, a higher profile will yield more volume and a larger increase in breast cup size. The profile refers to how far the implant projects from the chest and how much volume the implant will hold. A low profile implant will project the least distance from the chest, hold the least fluid, and is made to increase the breast about one cup size. The moderate profile will project farther, hold more fluid, and will generally give a two cup size increase. The high profile implant will project the most, hold the most fluid, and can increase the breast about three cup sizes. These generalizations reflect an average sized woman and can vary depending on how much breast tissue a woman has before augmentation.

| Low Profile | A low profile implant will project the least distance from the chest, hold the least volume, and is made to increase the breast about one cup size. |
| Moderate Profile | A moderate profile implant will project farther, hold more volume, and will generally give a two cup size increase. |
| High Profile | A high profile implant will project the most, hold the most volume, and can increase the breast about three cup sizes. |
As an example, an average breast will have a base diameter of about 12.5cm. For that base diameter, the low profile implant will hold 275cc, the moderate profile implant will hold 350cc, and the high profile implant about 425cc’s. These volumes may vary depending on the manufacturer and the type: saline or silicone. For saline implants, there is a recommended fill volume range such as 350 to 375cc’s. This means the manufacturer of the implant designed the implant to hold no less than 350cc’s and no more than 375cc’s. Underfilling the implant will result in more wrinkles or ripples in the implant which can distort the shape of the implant. Overfilling the implant will cause firmness as well as distortion. In addition, the implant warranty can sometimes be voided if the implant is filled to an incorrect volume. It is best to fill the implant to its maximum recommended volume because it will lessen the risk of implant rippling. For saline implants, it is best to choose the smallest appropriate implant (base diameter) filled to the maximum recommended volume. Silicone implants come prefilled and have no recommended volume range.
Generally, lower profile implant will have less upper pole fullness, less cleavage, and a more natural tear-drop look. In contrast, higher profile implants will have more upper pole fullness, more cleavage and an overall more augmented appearance. Because high profile implants will push the breast tissue and skin outward, the can effectively lift the breast making them useful in patients with more ptotic or droopy breasts.
CHOOSING A SIZE BEST SUITED FOR YOUR BODY TYPE
When choosing implant size, it is necessary to always choose an implant with the appropriate base diameter. Fear of going “too big” or “too small” can cause some women to choose a base width which might not fit their chest measurements. The choice is always with the profile and not the base diameter. Also, it is important to remember not to compare implant volumes between two patients. A 325cc implant might be small for a taller woman with a wider base width but be very large for a shorter woman with a smaller base. Accurate measurement of the base diameter is a reliable and sure way of finding the perfect implant size.
3D imaging to Assist in Implant Sizing
Perhaps the greatest source of anxiety in preparing for breast augmentation surgery is with implant size choice. Patients worry about looking too small, too large, or too fake. 3D imaging technology has revolutionized this process and taken most of the worry out of the planning process because patients can now visualize what a particular implant would look like on them.
Prior to 3D imaging, patients used a variety of methods to "size" or test implants. Before implants sizers, patients would use bags of rice measured to simulate a particular implant placed under a bra. Implant "sizers" were also used and placed over the breast, under a bra, to simulate size. The problem with these methods was that the appearance was often overestimated and the actual implant, when placed into the body under pressure, appeared much smaller. Women using sizers to pick an implant over complained that they were much smaller that the sizer had predicted.
3D imaging technology uses digital photographs or scanned images to generated a 3D model of the breast which then can be used to simulate what a particular implant would look like after augmentation. The imaging can be used to simulate implant volume, implant shape, and implant profile so that all variables can be simulated and controlled. The technology is web-based and extremely versatile for use both in the office during consultation, via a web based Online consultation, or even at the patient's discretion at home.

While these systems can help, it is important to remember that they are not perfect and should be used in the proper context. It is most important to review your surgeons credentials and before and after results.
IMPLANT PLACEMENT

The breast implant can be placed directly under the breast tissue (subglandular), under the chest muscle (submuscular), or in a combination procedure known as a “dual plane.”
| Subglandular Pocket | A subglandular pocket has less tissue coverage, more implant visibility, and a higher incidence of capsular contracture. It is useful in certain cases such as a tuberous breast deformity that rely on a more direct effect of the implant on the breast tissue. |
| Submuscular Pocket | A submusular pocket is most widely used. There is more tissue coverage, less implant visibility, and a lower incidence of capsular contracture. Placing an implant under the muscle can cause movement of the implant with chest muscle movement; animation deformity. |
| Dual Plane | A Dual Plane pocket is partially subglandular and partially submuscular. This approach is beneficial in cases with looser skin and a more droopy or ptotic appearance. The dual plane allows more perfect centering of the implant directly under the breast to prevent the implant from sitting too high in relation to the breast (double bubble). |
SUBGLANDULAR BREAST AUGMENTATION
Subglandular breast augmentation is not commonly used but is useful in certain cases where a more direct effect of the implant on breast tissue is needed such as a tuberous or constricted breast deformity.
Subglandular augmentation does not provide as much tissue coverage over the implant making the implant more palpable (easy to feel) and more visible. In thin patients, ripples in the implants are more visible with the subglandular approach. Because there is no muscle covering the implant, there can be a sharp demarcation around the edges of the implant, especially in the upper pole, causing an unnatural appearance.
There is also a higher incidence of capsular contracture (problematic scarring around the implant) with subglandular implants which can result in hard, painful, and distorted breasts. Because the implants sit on top of the chest muscle, there is minimal movement of the implant with chest muscle movement; animation deformity.
SUBMUSCULAR BREAST AUGMENTATION
Submuscular augmentation is most commonly used. Because there is more tissue covering the implant, there is less palpability and visibility of the implant and a more natural upper pole slope. In thin women, placing the implant under the muscle gives a more natural appearance by hiding the edges of the implant especially in the inner and outer parts of the breast. Because the muscle retains most of its attachments to the breast bone (sternum) and rib cage, there is more support for the implant which tends to decrease ptosis (sagging of the breast) over time. One of the major benefits of submuscular augmentation is that there is a 50% lower incidence of capsular contracture (scar tissue formation around the implant) using this approach.
Submuscular augmentation is slightly more painful and requires time for the implant to assume its final position. In the first several days ofter surgery, the muscle will be tight over the implant which pushes the implant upwards (riding high). Over time the muscle will stretch and relax so that the implant will lower itself into a more natural position.
DUAL PLANE BREAST AUGMENTATION
Dual plane breast augmentation allows for submuscular placement of the implant and creates release of the breast tissue above the muscle to allow the breast to position itself more directly over the implant and avoid a double bubble appearance. This technique is useful in cases of breast ptosis or pseudoptosis where the breast is somewhat droopy or ptotic such as occurs after childbirth and breast feeding.
INCISION PLACEMENT
There are four incisions which can be used in breast augmentation: Inframammary, periareolar, transaxillary, and umbilical. Incision choice will determine where on the body a permanent scar will be placed and can affect breast shape. The goal is to choose an incision which is least visible and permits the best access for precise implant placement.
| Inframammary or Breast Crease Incision | The most common incision, it is placed in the lower fold of the breast or breast crease so that the natural overhand of the breast will hide it from view. This allows the most direct access and precision when making the implant pocket. |
| Periareolar Incision | This incision is placed just inside the lower areola making it virtually imperceptible once healed. This does require incising through the breast tissue which causes internal scarring in the breast. Due to bacteria present in breast ducts, contamination of the implant is more likely with this approach which can lead to capsular contracture. |
| Transaxillary | Often referred to as "scarless" breast augmentation (no breast scar), the incision is placed into a skin fold in the axilla or armpit which usually heals very well. This is a more remote approach and precise control over the implant pocket dissection is more difficult. |
| PeriUmbilical | The most remote approach therefore least precise. Somewhat controversial and not widely practiced. |
INFRAMAMMARY
The inframammary incision (IMF) is placed in the lower fold in the breast so that the natural shape of the breast will hide it from view. Generally, this incision is small, about 3.0cm, and heals very well. This is the most common incision and allows the best visibility when dissecting the breast pocket for a more precise implant placement. There is minimal scarring to the breast tissue and less chance of bacterial contamination.
PERIAREOLAR
The periareolar incision is usually placed at the lower and middle part of the areola just inside the pigmented skin. This incision generally heals very well making it difficult to detect. This incision is useful when the inframammary crease needs to be adjusted such as when correcting a constricted or tuberous type breast deformity. It is also useful when the skin of the breast needs to be tightened with a periareolar breast lift/mastopexy.
The disadvantages of this incision are that the incision is placed on the most visible part of the breast. There can be damage to nerves which provide sensation to the nipple. Because this approach requires dissection through the glandular part of the breast, there can be internal scarring in the breast which can be problematic on screening mammograms. Lastly, there is a higher risk of infection with this approach because there are bacteria in the breast glands which can come into contact with the implant. Contamination of the implant can lead to capsular contracture or problematic scar tissue formation around the implant.
ENDOSCOPIC TRANSAXILLARY (TRANS AX OR ENDO)
This incision is placed in a skin fold in the armpit (axilla) which usually heals very well. Many proponents of this approach advertise it as “scarless breast augmentation.” While their intent is to convey the idea that there is no scar on the breast, the reality is that this approach is not scarless and the armpit scar is every bit as permanent as a breast scar. In most cases, it will heal very well but occasionally patients can develop unsightly scars in the armpit which will be visible in clothing which exposes the arm such as bathing suits, tank tops, dresses, etc.
Because this operation is done from a “top down” approach, the dissection is slightly different. There is less control over the pocket dissection which is done more bluntly which can result in more pain and bleeding. With the transaxillary approach, the inframammary crease or fold in released about a centimeter to make room for the implant. Over time this can result in an increased distance from the nipple to the inframammary crease giving the breast a rounder shape with the nipple in the center of the breast rather than a teardrop shape. The increased distance from the nipple to the breast crease can give the appearance of a bottom heavy or bottomed out appearance.
UMBILICAL
The umbilical or belly button approach is not commonly used because access to the breast is remote and difficult. Large tunnels are created in the subcutaneous fat over the abdominal muscles to gain access to the breast. In thin patients, this can result in ridging and contour irregularity of the abdomen. The dissection of the breast pocket is mostly done bluntly rather then precisely with surgical cauterizing instruments which can result in breast trauma, scarring, and bleeding. It is difficult to place the implant under the muscle using this approach. For these reasons, this approach is somewhat controversial and not widely practiced.
IMPLANT TYPES

| Saline | Saline implant are less viscous, feel less natural, and are more prone to rippling. They are the least expensive implant. |
| Silicone | Silicone implants are the most popular. They come in a variety of viscosities, feel more natural, and are less prone to rippling. They are sometimes referred to as Gummy Bear implants. |
| Structured Saline | Structured saline implants are made with multiple chambers. Although filled with saline, they have a look and feel more similar to silicone. They are popular with patients who desire saline implants but also want a more natural look and feel. |
SALINE
Saline implants are less viscous than silicone and thus feel less natural: like a waterbed. Saline implants will ripple more than silicone when filled to their recommended volume. Saline implants have a recommended volume range making them somewhat adjustable. This can be helpful in correcting differences in size between the breasts to give more perfect symmetry. If a saline implant deflates it will lose volume and be obvious. In contrast, silicone ruptures are less obvious as the silicone gel will stay relatively in place; silent rupture. Many patient prefer a more natural filling substance: saline. Saline implants are less expensive.
SILICONE
Silicone implants have become the standard for cosmetic breast augmentation since their FDA approval for patients over age 22 in 2006. Silicone implants have a softer and more natural feel. They tend to hold their shape better and have less rippling. The new generation silicone implants come in a variety of viscosities which do not leak if there is a compromise in the outer coating of the implant. However, because these implants do not deflate like a saline implant would do, it can be more difficult to detect if a rupture has occurred. For this reason, in cases of a suspected rupture, an breast MRI may be necessary to diagnose a rupture.
Because of the softer feel and less rippling, silicone implants are ideal for thin patients with small breasts. Silicone implants come “prefilled” and there is no control over the volume once the implants are removed from the sterile packaging.
Silicone implants also come in three different levels of cohesivity or viscosity. In general, the more cohesive an implant is the more it resists gravitational forces. More cohesive implants are more firm in feel. Highly cohesive implants will hold a round shape in the upright position giving a rounder look with more upper pole fullness and cleavage. Less cohesive implant have a softer feel and less upper pole fullness with a slightly more natural or teardrop appearance.

| Silicone: Least Cohesive | Least viscous silicone implant. Softest with less upper pole fullness. More natural appearance. |
| Silicone: More Cohesive | Moderate viscous silicone implant. Slightly more firm with more upper pole fullness. |
| Silicone: Most Cohesive | Most viscous silicone implant. Firmest with most upper pole fullness. |
STRUCTURED SALINE
Recently, a multi-chamber saline implant has been FDA approved for breast augmentation. This implant is manufactured as the Ideal Implant. This implant is marketed as a "structured implant" referring mulit-chamber baffle shells. The feels more similar to a silicone implant than a traditional saline implant. It also has a lesser degree of rippling with a lower deflation rate than normal saline implants.
TEXTURED and SMOOTH IMPLANTS

| Smooth Implant | Smooth implants are most commonly used and have a smooth silicone coat. No association with ALCL. |
| Textured Implant | Textured implants have a rough surface. They are designed to resist capsular contracture and adhere to tissue surfaces to prevent implant movement. Associated with ALCL (very rare). |
Most the above implant types come in either a textured or smooth coating. Smooth implants have a clear silicone surface. Textured implants have a "rough" surface which has been proven to reduce the risk of capsular contracture in subglandular augmentation. For submuscular augmentation, there is some debate as to whether textured implants reduce the risk of capsular contracture. Textured implants also hold their position in the pocket better than smooth implants making them more resistant to bottoming out. Bottoming out refers to an implant which sits low in the pocket due to the stretching of the lower pole skin over time. Because textured implants will not move or rotate, shaped or anatomic implants only come in the textured option.
In very rare cases, texture implants have been associated with Anaplastic Large Cell Lymphoma (ALCL). This extremely rare type of breast capsule cancer is cured with removal of the involved capsule.
IMPLANT SHAPES

| Round Implant | Smooth implants are most commonly used and have a smooth silicone coat. No association with ALCL. | |
| Shaped Implant | Textured implants have a rough surface. They are designed to resist capsular contracture and adhere to tissue surfaces to prevent implant movement. Associated with ALCL (very rare). |
Implants come in two shapes: round and shaped/anatomic. Round implants are most commonly used. Shaped implants are form stable meaning that they hold their shape against gravitational force. Shaped implants are designed to be tear dropped in appearance with less upper pole fullness and a thus a more natural breast shape. To limit the chance of rotation and possible deformity, shaped implants only come in the textured implant surface which is rarely associated with ALCL (see above). As an alternative, a lower profile, less viscous gel implant can closely mimic the tear drop shaped implant as gravity will pull the softer gel downwards limiting upper pole fullness.
Breast Augmentation Without Implants: Fat Grafting
For a variety of reasons, some women desire to have breast augmentation without using implants. While breast augmentation remains the most popular plastic surgery procedure with an overwhelmingly positive patient satisfaction rate, breast implants do have a few drawbacks including implant palpability, malposition, rippling or visibility animation deformity, capsular contracture, and the need to have implant replaced.
For these women, fat grafting is a good alternative to implants as a way to add volume to the breast. Fat is harvested using liposuction. This fat is specially treated and then re-injected into the breast to give a one to two cup size increase. While the majority of the transplanted fat survives and becomes permanent, some of the fat will be reabsorbed. When more augmentation is desired, the procedure may have to be repeated.
Dr. Burns is a nationally recognized expert in both fat grafting to the breast and implant based augmentation.
Rapid Recovery Breast Augmentation

Rapid Recovery Breast Augmentation represents several decades of advances in surgical technique. Historically, breast augmentation was associated with prolonged recovery and sustained discomfort. Surgical technique relied heavily on blunt dissection of the tissue which caused more trauma and bleeding.
Early range of motion was discouraged and patients were instructed to avoid activities of daily living for long periods of time. With rapid recovery breast augmentation, patients can expect a rapid return to work, daily activities, and even exercise.
The following principles are critical to helping patients quickly recover from breast augmentation with excellent outcomes.
- Before surgery: Patients need to be in good physical condition with no recent illness. Avoid smoking or any products which contain nicotine including vaporized devices. Avoid diet pills, herbal supplements, or aspiring containing products. Maintain a healthy diet and hydration before the procedure.
- Anesthesia: General anesthesia provided by an anesthesiologist is actually better for rapid recovery than "awake breast augmentation" which is done primarily by non board certified surgeons in a nonsterile and poorly controlled office environment. General anesthesia allows the anesthesiologist to safely control blood pressure and heart rate during the procedure which minimizes bleeding. Because there is no pain with general anesthesia, the muscle is more easily and less traumatically dissected and the implant placed without force. General anesthesia also relies more on anesthetic gases which are more quickly eliminated from the body. For these reasons, general anesthesia allows the patient to recover much quicker with less pain.
- Surgical technique: Surgical technique must be both precise and methodical. A skilled surgeon knows exactly how large to make the implant pocket and where each major blood vessel is located to prevent any bleeding or excess dissection. The majority of implants will be placed below the chest muscle (pectoralis major muscle). Dissecting the pocket to place the implant is done using cautery and not bluntly. Cautery under direct visualization minimizes bleeding and trauma to the tissue. The pocket should be carefully measured and made to the exact size of the implant. Great care should be taken to avoid any contact with the rib cage which can lead to pain and trauma. Before placing the implant a long lasting local anesthetic is placed into the muscle and breast to help with any discomfort from stretching of the tissue for the first 72 hours. For implant placement, we use a funnel and a no touch technique to avoid trauma to the patient, the implant, and to maintain sterility. It is important that the implant is placed only one time and avoid taking the implant in and out of the pocket. This avoids contamination and any additional trauma to the breast.
- Post surgical care: All sutures are placed below the skin meticulously lining up the incision edges to optimize the quality of the scar. The skin is then sealed to keep out water and covered with sterile surgical tape which will stay in place for two weeks. There are no sutures to remove, no drain tubes, and no need to care for the incision as it will be sealed and covered. The incision is also numbed with a long acting local anesthetic so that it should be pain free for at least 48 hours. Patients can shower the night of surgery if they wish. Each patient is sent home with a soft and comfortable surgical bra which is worn for the first week. There are no tight wraps, surgical dressings, and overly tight garments. Patients can begin wearing normal clothing and bras within a week.
- Implant choice: Obviously, the more stretching that occurs the more pain a patient will feel. Placing a very large implant will stretch the tissue and cause more pain than a smaller implant which does not put much stretch on the tissues. In other words, going from an A to D will be more painful than going from A to B. However, even with larger implants, rapid recovery is still possible and can be expected.
- Medication choice: While patients may request narcotic pain medication, most patients can rely on non steroidal type pain medications (NSAIDS). This antiinflammatory pain medication allows quicker recovery and decreases negative side effects such as sleep disturbances, decreased mental clarity, and constipation. The addition of long lasting local anesthetic in surgery, Exparel, decreases the need for post surgical pain medication.
- Early return to activity: Patients are encouraged to engage in normal activities of daily living such as showering, drying their hair, and arm movement. Return to work is generally possible within 2 or 3 days. Light exercise such as treadmill walking, spin class, or elliptical trainer is possible within a week. More aggressive exercise such as weight training, yoga, Barre classes, jogging, or Crossfit can be resumed in 4 to 6 weeks.
Following these guidelines, rapid recovery from breast augmentation is possible in almost every case. Choosing an experienced Board Certified Plastic Surgeon who specializes in Breast Augmentation is important for both rapid recovery and obtain the best aesthetic outcome.
Photo Galleries and Results
Before and after photos are categorized by size and breast shape.
Breast Augmentation by Cup Size
If increasing your cup size is your goal, you have many options available to you. If you’re starting with an A-C cup size, you can grow to any size, but the process will change slightly depending on how much growth you desire. Small growth changes (like from A cup to B cup) require a low-profile implant, while intermediate changes (from A cup to C cup) require a moderate or moderate-plus implant. For the greatest change (from A cup to D cup), a high-profile implant will be used.

|

|

|
| A cup to B cup | A cup to C cup | A cup to D cup |

|

|

|
| B cup to C cup | B cup to D cup | C cup to D cup |

|
| D+ cup |
Breast Augmentation by Breast Shape





Dallas plastic surgeon Dr. John Burns, a member of the prestigious Dallas Plastic Surgery Institute and a nationally-recognized expert in breast enhancement, welcomes the opportunity to discuss breast augmentation and other cosmetic goals with you. To make an appointment, simply call his office at 214-515-0002, or send an email through his website. Online consultations are also available. Dr. Burns and his staff look forward to meeting you!